
What is ankle impingement?
Ankle impingement is characterised by abnormal abutment of excessive soft tissue or bone, during normal ankle movement, resulting in pain. The pain is caused by a mechanical obstruction to movement.
Ankle impingement is typically described based on the location of the ‘impingement’ and the underlying cause.
- Anterior Ankle Impingement
- Posterior Ankle Impingement
Anterior Ankle Impingement
Anterior ankle impingement is one of the most common ankle presentations seen by orthopaedic surgeons. ‘Anterior’ refers to the region at the front of the ankle joint.
Relevant Anatomy
The ankle joint is made up of the lower end of the tibia (shin bone) and fibula, which both articulate with the talus bone.
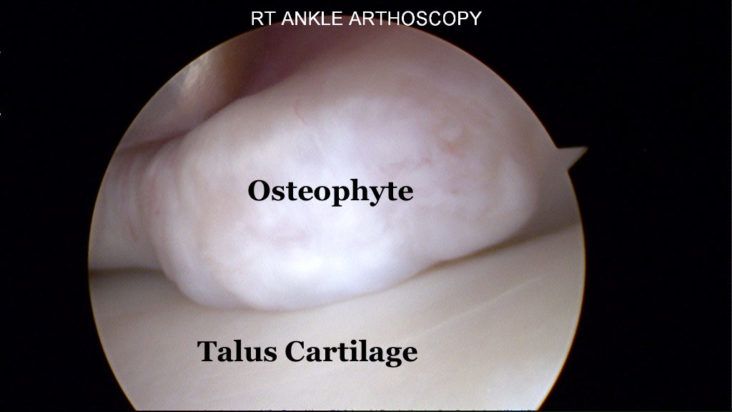
In the normal ankle joint, there is an anterior recess or space, that allows the ankle to ‘dorsiflex’ without any mechanical obstruction. When there is excessive soft tissue scarring or bone formation (‘osteophytes’) in this space, the ankle is unable to move freely, and ‘impingement’ occurs with resultant pain and stiffness.

Bony Impingement
Anterior Bony impingement is characterised by the formation of spur ‘osteophytes’ at the front of the lower tibia. This is a common condition in athletes with repetitive ankle dorsiflexion, such as football players, soccer players, ballet dancers, and runners. Repetitive micro trauma to the cartilage at the front of the tibia results in progressive scar cartilage (fibrocartilage) formation and ‘osteophytes’. These osteophytes can ‘break off’ and become loose bodies within the ankle joint.
Soft Tissue Impingement
Anterior soft tissue impingement is usually the result of recurrent ankle sprains (inversion injuries). Chronic inflammation and scarring of the synovial lining results in soft tissue entrapment within the front of the ankle joint.
Bassett’s ligament is a thickening of the lower part of the Anteroinferior tibiofibular ligament (AITFL). While it may be present in normal ankle joints, this ligament can also result in ‘impingement’ during ankle movement.

Diagnosis
Patients typically present with pain at the front of the ankle joint, which is made worse with ankle ‘dorsiflexion’ movements. These include walking uphill, running, landing from a jump, and pushing the brake of a car. A history of recurrent ankle sprains is often present.
Examination will provoke pain at the front of the ankle joint with forced dorsiflexion.
Typically a weight bearing x-ray and MRI scan are performed. Bone impingement is visualised on the plain x-rays as anterior spurring on the lower end of the tibia. Soft tissue impingement requires a MRI scan for visualisation.

Treatment
In patients that have failed conservative measures, a keyhole arthroscopic ‘decompression’ is typically offered. This allows direct visualisation of both soft tissue and bony causes for impingement, and clearance of these structures can be performed.
Posterior Ankle Impingement
Relevant Anatomy
Posterior Ankle Impingement refers to abnormal abutment of excessive soft tissue or bone at the ‘back’ of the ankle joint. This ‘abutment’ occurs when the ankle is positioned in a plantar flexed position (such as is seen in ballet dancers).


The posterior aspect of the ankle region is made up of the ‘back’ of the tibia (shin bone), the ‘back’ of the talus, and the back of the calcaneus (Heel bone). The tendon to the big toe (FHL tendon) runs through this region, and can be irritated with this condition.
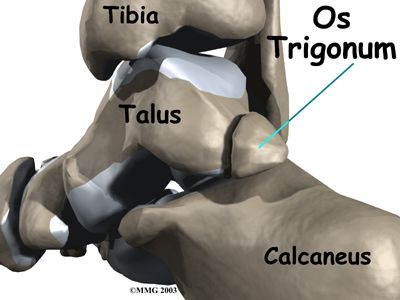
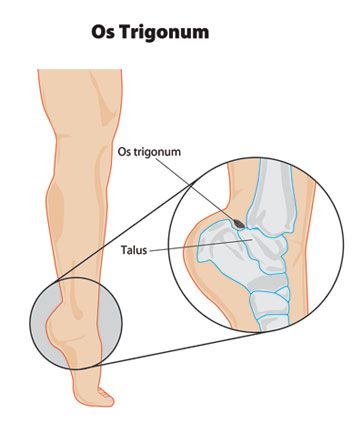
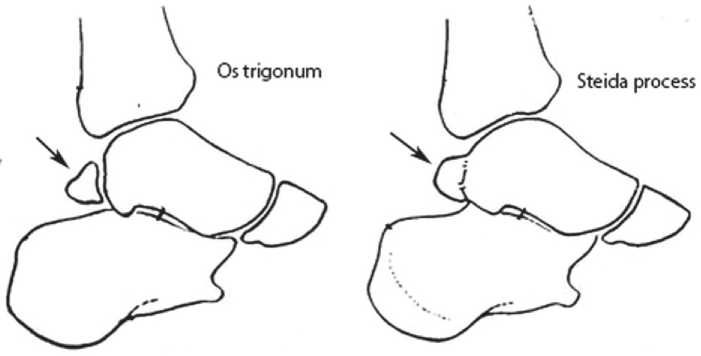
Os Trigonum
The most common cause of posterior impingement is the presence of an ‘Os Trigonum’. An ‘Os Trigonum’ is an un-united tubercle at the back of the talus. It is seen in up to 10% of the population, and often present in both ankles. Most patients with an Os Trigonum do not have any symptoms.
However, following either an ankle sprain, or repetitive plantar flexion, such as that experienced in ballet dancers, the Os Trigonum can cause irritation and pain at the back of the ankle.
Steida Process
Another form of bony impingement is seen in patients with a Steida Process. This represents an elongated tubercle (posterolateral) of the talus. Despite not have the ‘un-united’ section that is seen in the Os Trigonum, the same abutment of tissue occurs at the back of the ankle, resulting in pain.
Ankle Impingement – Making the diagnosis
Patients typically present with pain at the back of the ankle joint. This is exacerbated by repetitive plantar flexion activities. While this is classically described in Ballet dancers, whilst performing Pointe work, it can also be seen in many athletes during running and jumping activities.
A clinical examination is performed, including assessment of any posterior ankle impingement sign.
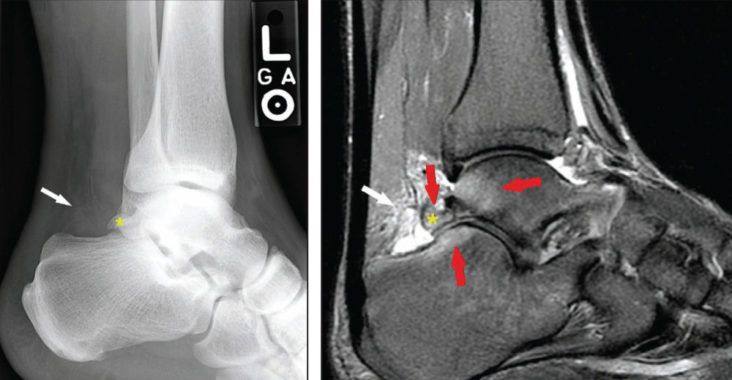
A plain xray will asses for the presence of an ‘Os Trigonum’ or ‘Steida Process’
A MRI scan confirms any associated soft tissue irritation and assess for high signal within the os trigonum.
Ankle impingement – Treatment
If conservative measures fail, posterior ankle impingement secondary to bony impingement from an os trigonum typically requires surgical removal to relieve symptoms. This is done via a keyhole posterior ankle arthroscopy, and the Os trigonum is removed.
It is performed as a day procedure, and immediate weight bearing is allowed.
A structured physiotherapy program is commenced to reduce postoperative scarring and the patient quickly returns to function, with resumption of running at 4-6 weeks.
Do you experience any of the following?
Frequent Ankle Sprains
Pain in your ankle
Swelling around your ankle